

Arrhythmia
- Atrial Premature Contraction / Ventricular Premature Contraction
- Ventricular Premature Contraction
- Paroxysmal Supraventricular Tachycardia
- Atrial Fibrillation
- Atrial Flutter / Atrial Tachycardia
- Ventricular Tachycardia
- Ventricular Fibrillation
- Bradyarrhythmias (Sick Sinus Syndrome, Atrioventricular Block)
What is Arrhythmia
Arrhythmia refers to a condition where the heartbeat becomes faster, slower, or irregular. You may be told ‘You have an arrhythmia’ during your annual health check-up or at a hospital examination. The term ‘arrhythmia’ encompasses a wide range of conditions, from those that can be left untreated to those that are life-threatening. These arrhythmias may be accompanied by symptoms such as palpitations, dizziness, or chest discomfort, or they may be completely asymptomatic. Don’t casually think, ‘I was told I have an arrhythmia, but I don’t feel anything, so I’ll leave it alone.’ Please consider visiting a hospital as an opportunity to review your health.
At the Cardiology Department and Arrhythmia Group of St. Luke’s International Hospital, experienced arrhythmia specialists are available to provide thorough consultations on all aspects of arrhythmia – what kind of arrhythmia you have been diagnosed with, what you should do in the future, and what treatment options are available.
Various Types of Arrhythmias
There are various types of arrhythmias, but the following are the most common ones. When you are told ‘You have an arrhythmia,’ try to find out which type of arrhythmia you have.
Atrial Premature Contraction / Ventricular Premature Contraction
Ventricular Premature Contraction
This is an arrhythmia where a single heartbeat occurs earlier than usual, often experienced as ‘skipped beats’ or ‘a momentary flutter.’ Almost everyone has this type of arrhythmia, so generally, observation alone is sufficient. However, if symptoms are severe or occur frequently, treatment may be considered.
Paroxysmal Supraventricular Tachycardia
This is an arrhythmia where the heart rate suddenly increases without warning, potentially causing strong palpitations or dizziness. Fortunately, it is rarely life-threatening, but because it can occur at any time and often has severe symptoms, treatment is recommended. There are types involving two pathways in the atrioventricular node or associated with WPW syndrome, and catheter ablation is considered particularly effective for treatment.
Atrial Fibrillation
This is an arrhythmia where the pulse becomes irregular or fast, and may be accompanied by symptoms such as palpitations, dizziness, or shortness of breath (it can also be asymptomatic). In recent years, with an aging society, the number of patients with atrial fibrillation has been increasing. While atrial fibrillation itself is rarely life-threatening, it can sometimes increase the risk of heart failure, and the biggest concern is the increased probability of stroke. If you are diagnosed with atrial fibrillation, be sure to consult with a doctor about appropriate treatment options.
For those diagnosed with atrial fibrillation and deemed at risk for stroke, it is generally necessary to take blood-thinning medication for life. However, there is a concern that making the blood thinner may increase the risk of bleeding complications.
At our hospital, we perform percutaneous left atrial appendage closure as a cardiac catheter treatment to enhance stroke prevention without relying on the strength of antithrombotic drugs. For more details, please see here.
Atrial Flutter
Ventricular Tachycardia
This is an arrhythmia that originates from the ventricles of the heart, causing the pulse to suddenly speed up, potentially leading to strong palpitations, chest pain, dizziness, or fainting. Ventricular tachycardia occurring in people with heart disease can be a cause of sudden death, making it highly dangerous. When ventricular tachycardia is observed, appropriate medical treatment is absolutely necessary.
Ventricular Fibrillation
This is an arrhythmia where the ventricles of the heart quiver in a fine, rapid manner, preventing the heart from pumping blood effectively, leading to cardiac arrest. It is the most dangerous type of arrhythmia, and when ventricular fibrillation is observed, immediate life-saving measures are necessary. If someone collapses in front of you and ventricular fibrillation is suspected, gather people around, call an ambulance, and quickly attach a nearby AED.
Bradyarrhythmias (Sick Sinus Syndrome, Atrioventricular Block)
These are arrhythmias where the pulse becomes extremely slow or the heart temporarily stops, which can cause symptoms such as shortness of breath, dizziness, fainting, or lead to heart failure. If symptoms are severe, treatment with a pacemaker may be necessary.
Arrhythmia Treatment
Our department offers a wide range of arrhythmia treatments, from drug therapy with antiarrhythmic medications to advanced treatments such as catheter ablation and device therapy. We provide high-quality St. Luke’s standard treatments tailored to each patient’s needs.
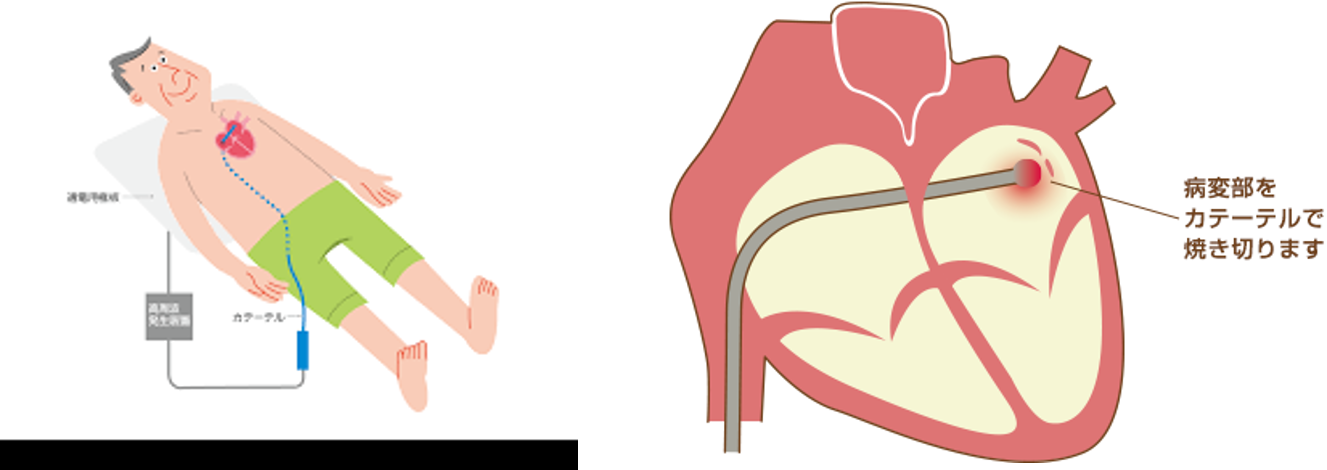
Catheter Ablation
Catheter ablation is a treatment method where a thin, long tube called a catheter is inserted through a blood vessel in the groin and guided to the heart. The catheter is used to locate the part of the heart muscle causing the arrhythmia and then ablate (destroy) that specific area. For certain types of arrhythmias, this can be a curative treatment, and we actively perform it at our hospital. The advantage of catheter treatment is that it is minimally invasive to the body, with only a small, inconspicuous incision. Patients can return to their daily lives soon after discharge.
Performance Record
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Atrial Fibrillation | 19 | 20 | 50 | 117 | 156 | 127 | 106 | 109 | 121 | 75 | 84 |
| Atrial Flutter | 9 | 21 | 25 | 15 | 10 | 17 | 16 | 7 | 7 | 6 | 9 |
| Atrial Tachycardia | 4 | 6 | 12 | 6 | 8 | 9 | 6 | 6 | 10 | 3 | 7 |
| Paroxysmal Supraventricular Tachycardia | 12 | 14 | 12 | 20 | 12 | 14 | 14 | 10 | 9 | 4 | 6 |
| WPW Syndrome | 9 | 2 | 12 | 6 | 7 | 6 | 10 | 5 | 3 | 1 | 1 |
| Ventricular Premature Contraction | 3 | 6 | 12 | 15 | 22 | 18 | 11 | 8 | 5 | 2 | 7 |
| Ventricular Tachycardia/Ventricular Fibrillation | 4 | 4 | 7 | 3 | 1 | 7 | 3 | 1 | 1 | 0 | 2 |
| Others | 0 | 2 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 |
| Total | 60 | 75 | 130 | 183 | 216 | 198 | 167 | 146 | 156 | 91 | 117 |
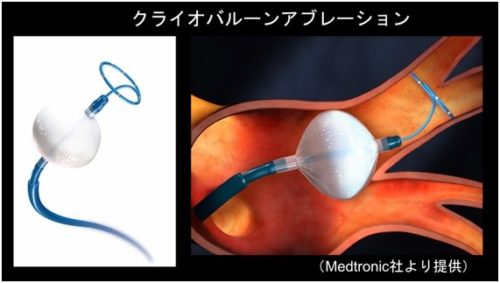
Cryoballoon Ablation
In addition to the conventional radiofrequency ablation that uses heat to ablate heart muscle, there is also a method called cryoablation that uses cooling for treatment. In our department, we actively use cryoballoon ablation, especially for atrial fibrillation ablation. While it’s difficult to say which is superior between radiofrequency ablation and cryoablation, we choose cryoballoon ablation based on the patient’s condition and heart shape, as it allows for safe and reliable creation of ablation lesions.
Device Therapy
Electronic devices implanted in the body for diagnosis or treatment of arrhythmias are called ‘devices.’ There are various types of devices, and we actively use them in our department, selecting the appropriate one based on the patient’s condition.
Performance Record
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pacemaker | 58 | 55 | 72 | 45 | 62 | 82 | 67 | 57 | 77 | 72 | 66 |
| Leadless Pacemaker | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 0 |
| Implantable Cardioverter Defibrillator (ICD) | 9 | 10 | 9 | 8 | 3 | 13 | 11 | 10 | 12 | 14 | 5 |
| Subcutaneous Implantable Cardioverter Defibrillator (SICD) | 0 | 0 | 0 | 0 | 0 | 4 | 6 | 5 | 2 | 4 | 6 |
| Cardiac Resynchronization Therapy Pacemaker (CRTP) | 1 | 2 | 2 | 1 | 3 | 2 | 0 | 3 | 3 | 2 | 1 |
| Cardiac Resynchronization Therapy Defibrillator (CRTD) | 2 | 10 | 7 | 3 | 2 | 5 | 1 | 2 | 4 | 3 | 6 |
| Implantable Cardiac Monitor (ICM) | 2 | 3 | 4 | 6 | 2 | 2 | 1 | 9 | 9 | 5 | 6 |
| Others | 0 | 0 | 0 | 3 | 1 | 4 | 5 | 3 | 1 | 2 | 2 |
| Total | 72 | 80 | 94 | 66 | 71 | 113 | 93 | 89 | 108 | 103 | 93 |
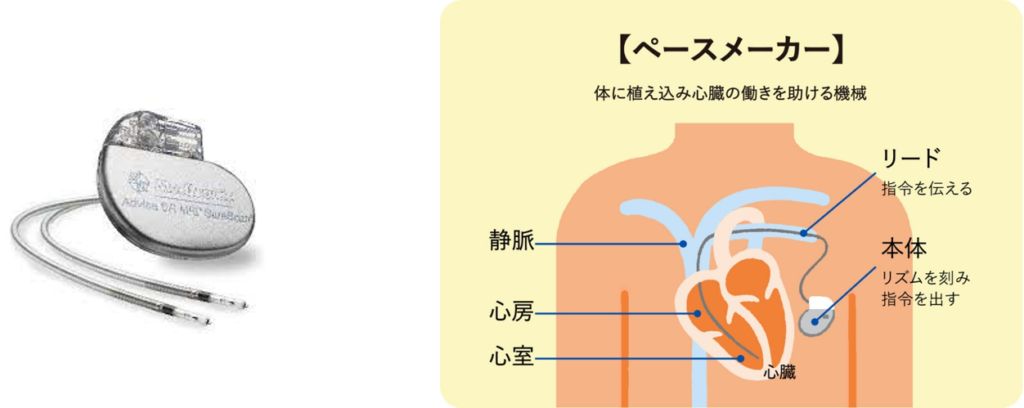
Pacemaker
Used for bradyarrhythmias such as sick sinus syndrome or atrioventricular block. When bradyarrhythmias cause the pulse to slow down or the heart to temporarily stop, symptoms such as shortness of breath, dizziness, or fainting may occur. Implanting a pacemaker can assist the slowed heart, potentially improving symptoms. In recent years, MRI-compatible types have become mainstream.
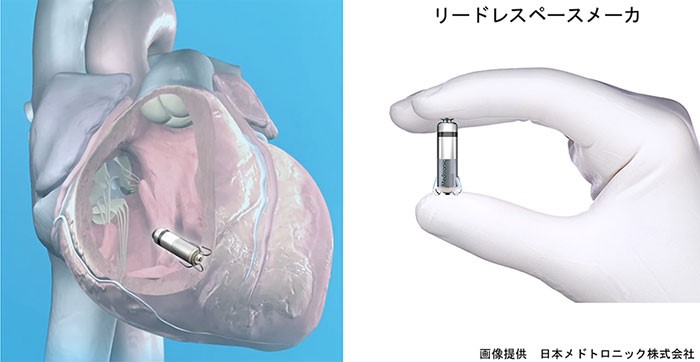
Leadless Pacemaker
This system directly places only the pacemaker body inside the heart. It has advantages such as lower risk of infection as it doesn’t use leads, and its use has been expanding in recent years.
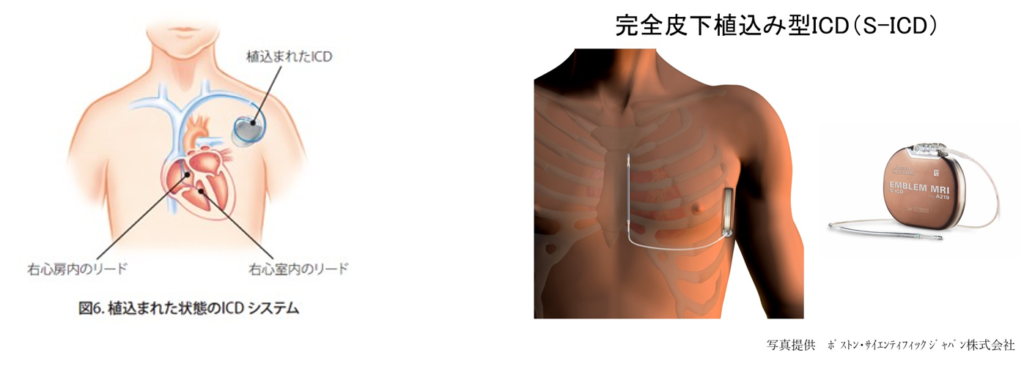
Implantable Cardioverter Defibrillator (ICD)
Life-threatening arrhythmias such as ventricular tachycardia and ventricular fibrillation can cause the heart to contract abnormally fast or quiver, potentially leading to cardiac arrest and sudden death. An implantable cardioverter defibrillator is considered the most effective method to prevent sudden death from such life-threatening arrhythmias. An implantable cardioverter defibrillator also includes pacemaker functions.
Subcutaneous Implantable Cardioverter Defibrillator (SICD)
Conventional implantable cardioverter defibrillators were transvenous types directly inserted into blood vessels and the heart, but recently, subcutaneous types where the body and leads are implanted under the skin of the chest have become available. Subcutaneous implantable cardioverter defibrillators have the advantage of being relatively easy to remove in case of infection complications, but they lack pacemaker functions, so they are used selectively based on the patient’s condition.
Cardiac Resynchronization Therapy (CRT-P, CRT-D)
In cases where heart failure occurs due to ‘dyssynchrony,’ a condition where the ventricular muscles contract out of sync, treatment with a biventricular pacemaker can potentially improve heart failure. Biventricular pacing is also called ‘cardiac resynchronization therapy.’ A device that combines biventricular pacing (CRT-P) with implantable cardioverter defibrillator (ICD) functions is called a cardiac resynchronization therapy defibrillator (CRT-D) and may be used for patients with severe heart failure.
Implantable Cardiac Monitor (ICM)
This is a device used for diagnosing the cause of syncope or stroke. A small device about 1cm x 5cm is implanted under the skin in front of the heart. The implantable cardiac monitor continuously monitors heart rhythms 24 hours a day, allowing for the actual recording of transient arrhythmias that are not usually observed.

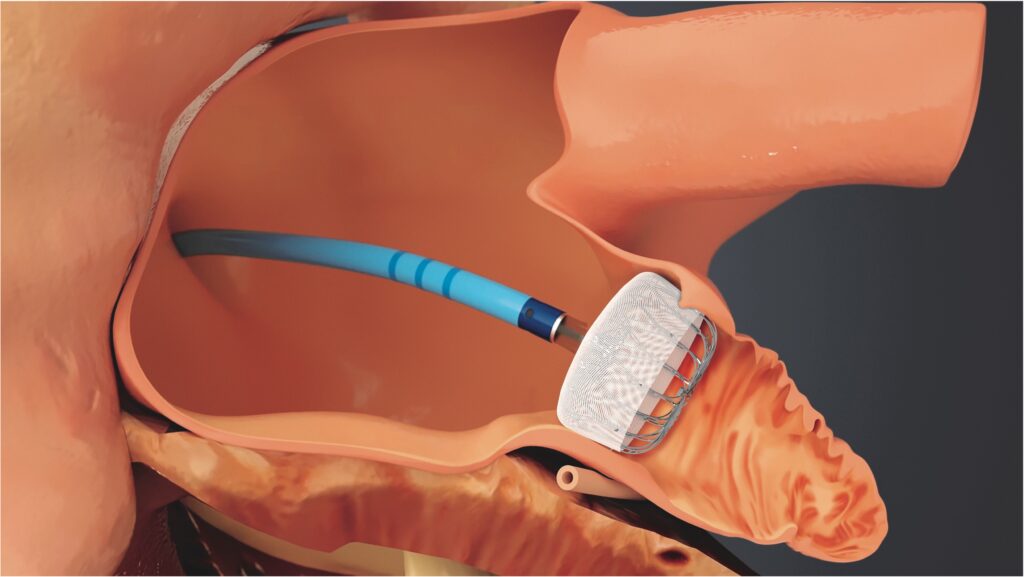
Cardiac Catheter Treatment to Prevent Stroke
The heart works as a pump to send blood throughout the body, affecting cerebral circulation as well. The heart and brain are organs with an extremely strong relationship. ‘Atrial fibrillation’, one type of arrhythmia, is known to be a cause of stroke, particularly in older individuals.
After a stroke, it is common to take antithrombotic medications to prevent recurrence by thinning the blood. In recent years, cardiac catheter treatments that enhance stroke prevention effects without relying on the strength of antithrombotic drugs have become available in Japan.
The catheter treatment for stroke prevention in patients with atrial fibrillation is called ‘percutaneous left atrial appendage closure‘.
This treatment is for the ‘prevention’ of stroke. As it is a preventive treatment, it is important to fully understand its purpose and effects before choosing this treatment, and the choice not to undergo catheter treatment should also be respected. We can provide consultations for those who just want to hear about the content and explanation of this treatment.
For more details, please see here.
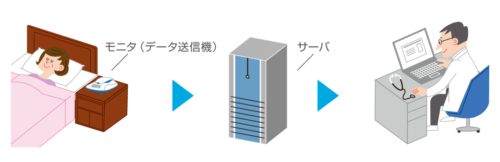
Remote Monitoring
Patients who have undergone device therapy need to regularly visit the device outpatient clinic to follow up on the device’s operation status and battery life. In recent years, remote monitoring, which allows device checks to be performed at home by placing a communication device at the bedside, has become widespread, and we actively implement it in our department. By introducing remote monitoring, it is possible to reduce the number of hospital visits and detect device malfunctions or dangerous arrhythmias earlier.
Short Hospital Stay, Minimally Invasive Treatment
Our department strives to complete treatments with the shortest possible hospital stay. For catheter ablation, we aim for a 1-night 2-day stay (treatment on the day of admission, walking discharge the next day). For device implantation surgeries, we standardize a 2-night 3-day stay for new implants and a 1-night 2-day stay for replacements.
We also make efforts to minimize patient burden, such as using sedatives during surgery, avoiding urinary catheters, and using cardiac CT instead of transesophageal echocardiography for pre-ablation thrombus checks (Note: This may not always be possible depending on the patient’s condition). When discussing treatment with your doctor, feel free to ask about your preferred inpatient treatment options.

